Research Shows EPA and Prozac Have Comparable Effects on Depression, Anxiety, and Neuroinflammation and the Clinical Case for Addressing Neuroinflammation in Psychiatric Assessment and Treatment Approaches
EPA, Inflammatory Physiology, and the Research Most Clinicians Aren’t Integrating into their Treatment Protocols yet
Many people navigating depression, chronic anxiety, persistent fatigue, cognitive fog, or emotional dysregulation spend years working exclusively within a psychological framework, which is absolutely appropriate and often necessary. Therapy, trauma processing, nervous system regulation, and relational repair are all genuinely important dimensions of healing. And at the same time, modern research continues to surface evidence that emotional and cognitive symptoms are also profoundly shaped by physiology, inflammatory load, nutritional status, and the quality of raw structural materials available to the brain and nervous system.
This blog post expands upon one of those findings, one that I sincerely feel deserves far more attention in mainstream wellness and mental health assessments and considerations than it currently receives.
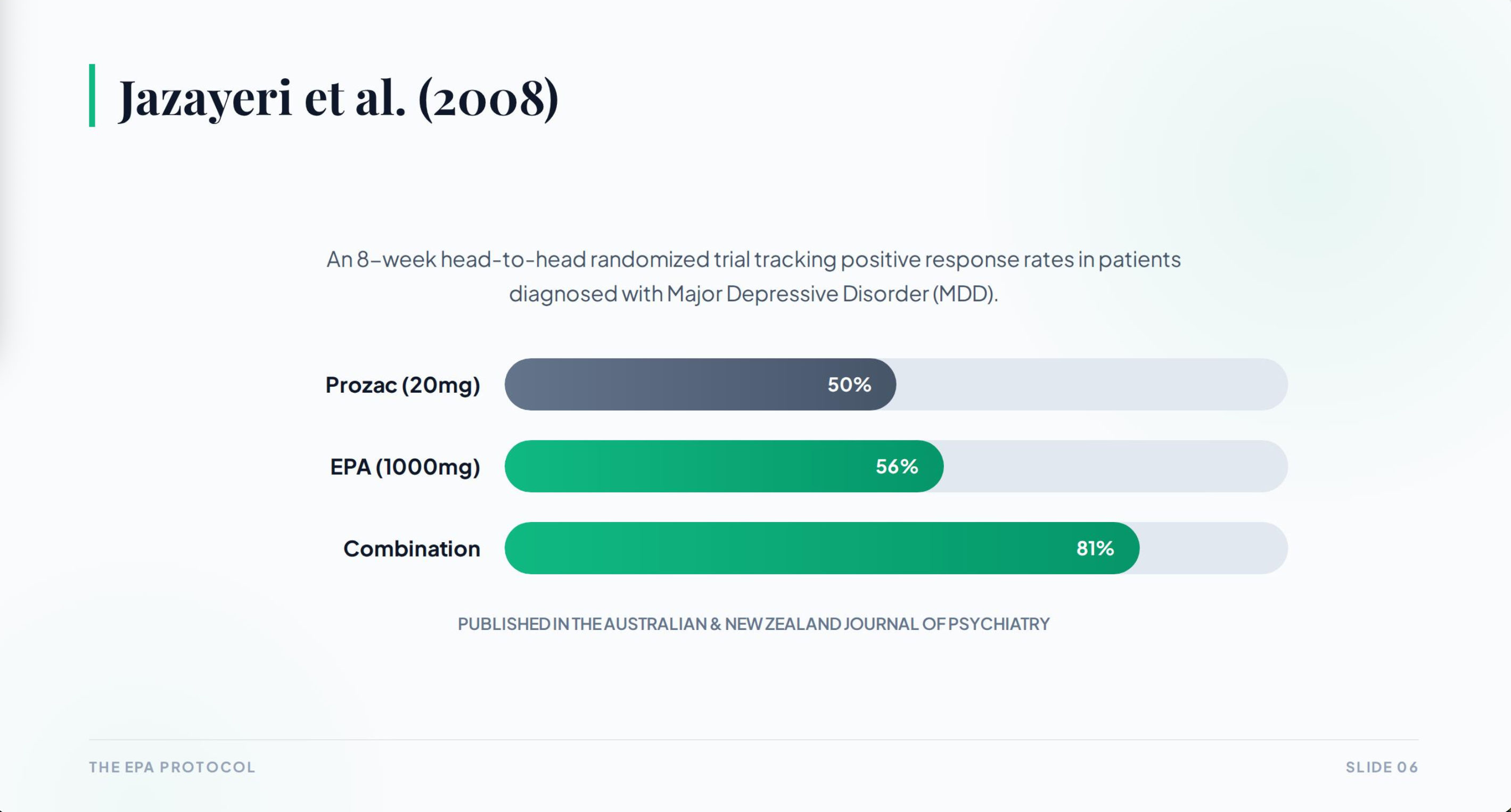
A peer-reviewed clinical trial published in the Australian & New Zealand Journal of Psychiatry found that 1000mg of EPA daily produced outcomes comparable to 20mg of fluoxetine, commonly known as Prozac, in patients with major depressive disorder over an 8-week period. The EPA group showed a 56% response rate. The Prozac group showed a 50% response rate. And the group receiving both together showed an 81% response rate. These are significant numbers. They suggest that EPA's anti-inflammatory effect on the central nervous system is producing measurable clinical outcomes that parallel those of a standard antidepressant dose, which has direct implications for how nutritional status is factored into psychiatric and functional medicine care and interventions.
In this blog, I’m going to walk you through what the research actually shows, why it makes biological sense, how it connects to what we understand about the gut-brain axis and neuroinflammation, and how that translates practically for people who are carrying significant emotional or physiological burden and are looking for research-grounded approaches to address the inflammatory and nutritional dimensions of that burden.
I am a Somatic nervous system coach and mindfulness researcher trained at the Polyvagal Institute, not a doctor or nutritionist. Nothing in this post constitutes medical advice, a recommendation to alter or discontinue any medication, or a clinical protocol. This is educational exploration grounded in peer-reviewed literature, and I encourage anyone considering supplementation or changes to their health practices to consult their provider.
Why the Brain Needs Fat to Function
The brain is approximately 60% fat by dry weight.The structural architecture of every neuron, every cell membrane, every myelin sheath wrapping the axons that carry signals across your nervous system depends on the availability and quality of dietary lipids. Cell membranes require specific fatty acids to remain fluid, permeable, and functionally responsive. Neurotransmitter receptors are embedded within those membranes. The speed and fidelity of neural signaling is directly influenced by the lipid composition of the tissue through which signals travel.
This is important because modern diets are significantly depleted in the kinds of fats the brain depends on. The industrialization of the food supply over the last several decades has shifted the average dietary fatty acid profile away from long-chain omega-3s like EPA and DHA toward highly processed seed oils and refined carbohydrates. The omega-6 to omega-3 ratio in ancestral diets is estimated to have been somewhere between 1:1 and 4:1. In contemporary Western diets, that ratio is often estimated at 15:1 or higher. This shift has consequences not only for cardiovascular health and metabolic function but for the structural and regulatory capacity of the central nervous system itself.
EPA, eicosapentaenoic acid, is one of the primary long-chain omega-3 fatty acids found in fatty fish and high-quality fish oil. It is distinct from DHA in its anti-inflammatory profile and its particular relevance to mood regulation. While DHA is more structurally concentrated in brain tissue, EPA appears to have a more pronounced effect on the inflammatory processes that underlie a significant portion of what we clinically recognize as depression and anxiety. Understanding why requires a brief look at the neurobiology of inflammation.
The Inflammatory Dimension of Depression and Anxiety
One of the most significant paradigm shifts happening within psychiatry and neuroscience over the past two decades is the growing recognition that depression and anxiety are not purely neurotransmitter disorders. The serotonin hypothesis, while historically useful, has never been a complete picture of what’s taking place in the brain and body of someone experiencing major depression or chronic anxiety. What research has increasingly revealed is that inflammatory processes play a central and often causally upstream role in shaping the neurobiological conditions associated with these states.
Inflammatory cytokines, the signaling proteins produced by the immune system in response to perceived threat, tissue damage, infection, or chronic stress, have direct effects on serotonin and dopamine metabolism, HPA axis activity, mitochondrial energy production, sleep architecture, and the brain regions involved in threat detection and emotional regulation. Elevated cytokine levels, particularly TNF-alpha, IL-6, and CRP, have been found consistently in individuals with treatment-resistant depression and chronic anxiety, suggesting that for a meaningful subset of people, the depressive state is being maintained in part by an inflammatory physiological substrate.
This is not to reduce depression or anxiety to a purely biochemical event separate from psychological history, relational context, trauma, grief, or lived experience. It is intended to acknowledge that the body and the brain are not separate systems, and that the physiological environment within which emotional experience is processed continuously influences its intensity, duration, and the nervous system's capacity to recover from it.
When inflammatory cytokines are elevated, the brain operates differently. Serotonin precursor availability is reduced because the enzyme IDO, activated by inflammation, redirects tryptophan away from serotonin synthesis and toward a pathway that produces neurotoxic byproducts including quinolinic acid. Dopamine synthesis and signaling are similarly affected. The prefrontal cortex, involved in cognitive flexibility and emotional regulation, shows reduced functional connectivity. The amygdala and anterior insula, involved in threat detection and interoceptive alarm, become more reactive. This is the neurobiological profile associated with persistent anxiety, chronic low mood, anhedonia, hypervigilance, cognitive fog, and emotional rigidity.
EPA acts directly within this inflammatory landscape. It serves as a precursor to anti-inflammatory eicosanoids and specialized pro-resolving mediators, bioactive lipids that actively signal immune resolution and dampen the cytokine cascades driving neuroinflammation. It competes with arachidonic acid, the precursor to pro-inflammatory eicosanoids, for the same enzymatic pathways, and its presence in sufficient quantities meaningfully shifts the overall inflammatory balance within the central nervous system.
This is the biological mechanism that gives the EPA and fluoxetine comparison its coherence. Fluoxetine increases serotonin availability by inhibiting its reuptake. EPA reduces the inflammatory burden that is suppressing serotonin synthesis and degrading the neurobiological environment within which emotional regulation is possible in the first place. They address adjacent but distinct dimensions of the same problem, which is also why the combination in the Jazayeri study produced the most substantial clinical response.
What the Research Shows and Helps us Understand
The core study I keep returning to, and that I've discussed extensively in my video content on this topic, is the Jazayeri et al. 2008 randomized controlled trial comparing 1000mg of EPA daily to 20mg of fluoxetine daily in patients with confirmed major depressive disorder over eight weeks. The trial was conducted rigorously, with blinded outcome assessment and standardized depression rating scales, and it found no statistically significant difference in response rates between the EPA and fluoxetine groups, while finding that the combination of both produced response rates of 81% compared to 56% for EPA alone and 50% for fluoxetine alone.
This finding does not mean EPA is a replacement for antidepressant medication in all contexts. That is not what the research claims, and it’s not what I am claiming either. What it does mean is that the therapeutic relevance of EPA in the context of depressive disorders is clinically measurable and comparable in magnitude to a commonly prescribed pharmaceutical at a specific dose. That’s a significant finding that deserves to be understood and discussed clearly.
The Peet and Horrobin 2002 dose-ranging study adds important specificity to the picture. Researchers tested 1g, 2g, and 4g of EPA daily in patients with depression and found that only the 1g dose produced significant improvement over placebo. Higher doses did not. This dose-specificity is biologically important and practically relevant because it support that more is not always better. The 1000mg threshold appears to be where EPA's anti-inflammatory and mood-regulatory effects are most pronounced, at least within this clinical context.
A 2019 meta-analysis published in Translational Psychiatry aggregating data from multiple randomized controlled trials found that omega-3 supplementation, particularly EPA-dominant formulations, produced meaningful reductions in depression symptoms compared to placebo, with the strongest effects in populations with elevated baseline inflammatory markers. The 2024 study referenced in my slide series extended* this finding by specifically identifying individuals with elevated hs-CRP levels (at or above 1 mg/L) as the subgroup showing the most dramatic antidepressant response to EPA supplementation, which reinforces the idea that EPA is particularly therapeutic in what researchers have termed "inflammatory depression."
These are well established findings that appear in peer-reviewed publications cited by leading researchers and discussed extensively by clinicians and science communicators including Andrew Huberman, a Tenured Associate Professor of Neurobiology and Ophthalmology at Standford University. Conducting randomized controlled trials in nutritional psychiatry presents distinct challenges, and ongoing debates regarding methodology, dose standardization, and individual variability exist. However, the convergence of mechanistic science and clinical outcomes linking EPA to the reduction of neuroinflammation is substantial, providing a compelling foundation for clinical consideration
The Gut-Brain Axis and How This All Connects
Understanding EPA's neurological relevance becomes even clearer when you place it within the broader context of the gut-brain axis, which describes the continuous bidirectional communication network connecting the gastrointestinal tract and the central nervous system through the vagus nerve, immune signaling, microbial metabolites, inflammatory cytokines, hormones, and neurotransmitter precursors.
Approximately 80 to 90 percent of vagal signaling travels afferently, meaning upward from the body to the brain (bottom-up.) The brain is continuously receiving real-time information about the physiological state of the gut, immune system, and visceral organs, and it organizes emotional tone, stress sensitivity, cognitive flexibility, and threat perception around those incoming signals. This is part of why chronic gastrointestinal inflammation or dysbiosis so often presents alongside anxiety, depression, fatigue, and cognitive fog. The inflammatory signals are traveling directly into the brain's regulatory architecture.
In addition, a significant proportion of the body's serotonin precursors are produced in the gut, where the microbiome plays an indirect yet meaningful role in neurotransmitter metabolism, HPA axis regulation, and immune modulation. When our gut microbial balance is disrupted by ultra-processed diets, chronic stress, repeated antibiotic exposure, sleep deprivation, or environmental toxin load, the downstream effects on nervous system regulation and mood can be substantial. And when dietary quality degrades and omega-3 status falls, the inflammatory baseline throughout the gut-brain axis tends to rise correspondingly.
This interconnection is why addressing EPA status is not an isolated nutritional intervention when you understand the underlying biology. Rather than simply adding a molecule to a deficient system, you’re providing anti-inflammatory structural materials to a communication network that’s influencing mood, cognition, autonomic regulation, and emotional resilience continuously from the bottom up.
How to Source EPA Effectively
Quality matters significantly with fish oil supplementation, and not all products deliver what their labels claim. The fish oil market contains a wide range of product quality, from highly concentrated, well-sourced formulations to low-potency products that would require six to eight capsules per serving to reach a meaningful daily dose of EPA.
There are a few things to look for when evaluating a fish oil product for therapeutic use. The EPA content should represent at least 60% of the total omega-3 volume per serving, because many standard fish oils contain a mix of EPA and DHA and may deliver only 180 to 300mg of EPA per capsule. The oil itself should remain structurally intact, meaning it hasn’t been heavily refined or oxidized, which is a quality concern with lower-grade products that can actually introduce inflammatory byproducts rather than reducing inflammation. Liquid fish oils and high-potency soft gels both have their place depending on preference and lifestyle.
Two products I use personally and recommend through my practice are linked below. I highly recommend cycling between the two for variation to maintain continual progress and avoid plateaus. I use one in liquid form and one as a high-potency soft gel, and I have found that having both available makes consistency easier depending on the day, how and what I'm eating, and what my routine looks like. Both meet the sourcing and potency standards I described above.
These are affiliate links, which means I receive a small commission if you purchase through them. I only share products I have personally explored and found meaningful enough to include in my work.

A Note on Chia Seeds, Hydration, and Brain Health
I want to share one additional practice that I consistently use and recommend and that connects directly to this same area of brain health, omega-3 support, and gut integrity, and that is rehydrated chia seeds in high quality mineral water.
Chia seeds are one of the most concentrated plant-based sources of alpha-linolenic acid (ALA), the short-chain omega-3 that the body can partially convert to EPA and DHA, though the conversion rate is modest and variable. They’re also an excellent source of soluble fiber, which supports microbiome diversity, short-chain fatty acid production, and intestinal barrier integrity. The fiber in chia seeds feeds beneficial bacteria in the large intestine that produce butyrate, one of the primary fuels for colonocytes and a compound with well-documented anti-inflammatory effects on the gut lining and immune system.
What makes rehydrated chia seeds particularly interesting is their gel-forming property. When chia seeds are soaked in water, they absorb up to ten times their weight in liquid and form a hydrophilic gel composed of soluble fiber. What makes rehydrated chia seeds particularly interesting is their gel-forming property. When chia seeds are soaked in water, they absorb up to ten times their weight in liquid and form a hydrophilic gel composed of soluble fiber. This gel is highly beneficial for individuals suffering from chronic constipation and sluggish bowel movements, as it directly restores optimal gut motility. Mechanistically, the gel adds bulk and heavy moisture to the stool, which mechanically triggers peristalsis - the rhythmic muscular contractions of the colon. This gel slows gastric emptying, lubricates the intestinal lining to resolve slow transit times, cleanses the walls of your intestines and colon from toxic accumulations and food debris, extends electrolyte absorption, and supports sustained cellular hydration in a way that drinking plain water alone can’t consistently achieve. The hydration benefits are slow-release rather than rapid-flush, which means the water and minerals are absorbed more gradually and retai
This is especially relevant for anyone living in a hot or dry climate, in the desert Southwest, or anywhere they’re sweating heavily during the summer months, because sustained hydration in those conditions requires more than volume intake. It requires the kind of slow absorption and cellular retention that electrolyte-rich gel structures support.
The formula I use and recommend is simple and straightforward. Add three to four tablespoons of organic chia seeds to 16 to 32 ounces of filtered water. Allow them to soak for at least 20 to 30 minutes, though leaving them to soak overnight produces the most complete gel. You can add a small pinch of mineral-rich salt – ranking them by decreasing mineral density, my top choices are Baja Gold, Celtic, and pink Himalayan salt – a squeeze of lemon, lime or citrus, and optionally a trace of raw honey if you want a light flavor. The resulting drink supports gut motility, microbiome feeding, cellular hydration, and omega-3 intake simultaneously, and it’s gentle enough for most digestive systems when introduced gradually, starting at one or two tablespoons of chia seeds.
For people navigating heat, dehydration-related fatigue, brain fog, or nervous system dysregulation in warm months, this is one of the simplest and most physiologically supportive practices available.
Situating the EPA Research Within a Multifactorial Picture of Mental Health
Human health is multidimensional, deeply individualized, and shaped continuously by trauma history, relational context, stress physiology, sleep, metabolic function, and the accumulated conditions of a lifetime. The latest neurobiological research highlights this complexity by revealing the foundational role that inflammation plays in mental health. Because of this multifactorial nature, addressing depression and anxiety requires a scope of understanding that goes far beyond basic supplementation or treating a simple nutritional deficiency state, though targeted biological support remains a critical piece of the puzzle. That complexity deserves to be held and considered. Research suggests that for a significant proportion of people carrying inflammatory burden alongside their emotional symptoms, the physiological substrate from which those symptoms are being generated is influenced in a measurable and clinically meaningful way by the availability of EPA within the central nervous system. When that availability is low and the inflammatory load is high, the neurobiological conditions for depression, anxiety, and dysregulation are reinforced from below.
When EPA status improves and neuroinflammatory tone decreases, the nervous system regains the structural capacity that was previously compromised.
Within the framework of the gut-brain axis, where inflammation, microbial health, vagal tone, stress physiology, and nutritional status continuously influence one another, EPA supplementation serves as a precise, upstream intervention. Rather than merely masking surface-level symptoms, this targeted input directly alters the foundational physiological conditions that shape their intensity and persistence, fitting seamlessly into a broader commitment to long-term physiological restoration.
For anyone navigating depression, chronic anxiety, persistent fatigue, or cognitive fog who hasn’t yet explored their inflammatory markers or omega-3 status, it may be worth having a conversation with your health provider about where those numbers sit. hs-CRP, a sensitive marker of systemic inflammation, can be checked through a standard blood panel. Omega-3 index testing, which measures EPA and DHA levels within red blood cell membranes, is available through several functional medicine labs and provides a direct picture of your tissue-level fatty acid status.
These are grounded, accessible interventions, that are increasingly well-supported by research that’s continuing to clarify the relationship between nutritional status, inflammatory physiology, and the brain's capacity to regulate emotional experience.
Closing Reflections
I’m sharing this research with you because I believe people deserve access to information that their standard medical encounters often don't have time to cover. This information doesn’t replace the care of a physician or therapist, and doesn’t suggest that a supplement will resolve what years of unprocessed experience, nervous system dysregulation, or chronic trauma have shaped. All of that said, understanding the physiological dimensions of emotional suffering is often meaningful and validating to people. It helps us recognize that our body is not a passive backdrop to psychological experience but an active participant in it, and that caring for our body with precision and attentiveness is itself a form of healing.
The gut, brain, immune system, microbiome, and autonomic nervous system are in continuous, bidirectional conversation, a complex system wherein the quality of available dietary fats serves as a foundational and structural pillar rather than a peripheral detail.
And the growing body of research around EPA, neuroinflammation, and mood regulation is beginning to make clear just how much that structural foundation influences what we experience, moment to moment, as our emotional and mental lives.
I am a Somatic nervous system coach and mindfulness researcher trained at the Polyvagal Institute. This post is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider before beginning any new supplement protocol or making changes to existing treatment.
Studies Referenced:
Jazayeri, S. et al. (2008). Comparison of therapeutic effects of omega-3 fatty acid eicosapentaenoic acid and fluoxetine, separately and in combination, in major depressive disorder. Australian & New Zealand Journal of Psychiatry, 42(3), 192-198. https://pubmed.ncbi.nlm.nih.gov/18247193/
Peet, M. & Horrobin, D.F. (2002). A dose-ranging study of the effects of ethyl-eicosapentaenoate in patients with ongoing depression despite apparently adequate treatment with standard drugs. Archives of General Psychiatry, 59(10), 913-919. https://pubmed.ncbi.nlm.nih.gov/12215080/
Liao, Y. et al. (2019). Efficacy of omega-3 PUFAs in depression: A meta-analysis. Translational Psychiatry, 9, 190. https://www.nature.com/articles/s41398-019-0515-5
Notes
*Available in this short video using this link.
Learn more about working with the gut-brain axis and nervous system health: [Gentle Offerings]
Join the community: Instagram @beautifulhumanhealing
Free Meditations on YouTube: @Dexterandalessandrina
